Health
National pharmacare – might it be a pig in a poke?

From the Macdonald Laurier Institute
By Nigel Rawson and John Adams for Inside Policy
No Canadian should have to choose between paying for medicines and paying for rent or food. National pharmacare has been proposed as a remedy to this situation.
“When will Canada have national pharmacare?” asks the author of a recent article in the British Medical Journal (BMJ). Better questions are: will Canadian pharmacare be the system many Canadians hope for? Or, might it turn out to be skimpy coverage akin to minimum wage laws?
In its 2024 budget document, the federal government proposed providing $1.5 billion over five years to support the launch of national pharmacare for “universal, single-payer coverage for a number of contraception and diabetes medications.” This has been hailed as a “big day for pharmacare” by some labour unions, patients and others, including the author of the BMJ article who said that national pharmacare should be expanded to cover all medication needs beginning with the most commonly-prescribed, clinically-important “essential medicines.”
In its budget, the government stated “coverage of contraceptives will mean that nine million women in Canada will have better access to contraception” and “improving access to diabetes medications will help improve the health of 3.7 million Canadians with diabetes.” Why not salute such affable, motherhood and apple pie, sentiments? The devil is in the details.
The plan does not cover new drugs for diabetes, such as Ozempic, Rybelsus, Wegovy, Mounjaro or Zepbound, all based on innovative GLP-1 agonists, where evidence is building for cardiovascular and weight loss benefits. This limited rollout seems based on cheap, older medicines, which can be less effective for some with diabetes.
The federal government has also consistently under-estimated the cost of national proposals such as pharmacare – not to mention other promises. In their 2019 election platform, the Liberals promised $6 billion for national pharmacare (the NDP promised $10 billion). Keen analysis shows that even these expansive amounts would be woefully inadequate to fund a full national pharmacare plan. This makes the $300 million a year actually proposed by the Liberals’ look like the skimpy window-dressing that it is.
National pharmacare, based on the most comprehensive existing public drug plan (Quebec’s), would cost much more. In 2017, using optimistic assumptions, the Parliamentary Budget Officer (PBO) estimated the cost for a national plan based on Quebec’s experience to be $19.3 billion a year. With more appropriate assumptions, the Canadian Health Policy Institute estimated $26.2 billion. In June 2019, the federal government’s own Advisory Council on the Implementation of National Pharmacare put the cost at $40 billion, while a few months later, the tax consulting company RSM Canada projected $48.3 to $52.5 billion per year. Five years later, costs no doubt have soared.
Even with these staggering cost a program based on matching Quebec’s drug plan at the national level would fail to provide anywhere near the level of coverage already provided to the almost two-thirds of Canadians who have private drug insurance, including many in unionized jobs. Are they willing to sacrifice their superior coverage, especially of innovative brand-name medicines, for a program covering only “essential medicines”? Put another way, are Canadians and their unions prepared to settle for the equivalent of a minimum wage or minimum benefits?
The PBO has estimated the cost of coverage of a range of contraceptives and diabetes medicines as $1.9 billion over five years, which is more than the $1.5 billion provided in the budget. However, this figure is based on an assumption that the new program would only cover Canadians who currently do not have public or private drug plan insurance, those who currently do not fill their prescriptions due to cost related reasons, and the out-of-pocket part of prescription costs for Canadians who have public or private drug plan coverage. This is major guesswork because existing public and private drug plans may see the new federal program as an opportunity to reduce their costs by requiring their beneficiaries to use the new program. If this occurs, the national pharmacare costs to the federal government, even for the limited role out of diabetes and contraceptives, would soar to an estimated $5.7 billion, according to the PBO.
Our governments are not known for accurate estimates of the costs of new programs. One has only to remember the Phoenix pay system and the ArriveCAN costs. In 2017, the Government of Ontario estimated $465 million per year to extend drug coverage to every resident under the age of 25 years. What happened? Introduced in 2018, prescriptions rose by 290% and drug expenditure increased to $839 million – almost double the guesstimate. In 2019, the provincial government back peddled and modified the program to cover only people not already insured by a private plan.
Although we believe governments should facilitate access to necessary medicines for Canadians who cannot afford their medicines, this does not require national pharmacare and a growing bureaucracy. Exempting lower-income Canadians from copayments and premiums required by provincial programs, as British Columbia has done, and removing the requirement to pay for all drugs up to a deductible would allow these Canadians access sooner, more simply, and more effectively.
Moreover, it isn’t just lower-income Canadians who want help with unmet medicine needs. Canadians who need access to drugs for diseases that are difficult to treat and can cost hundreds of thousands of dollars per year also require assistance. Few Canadians whether they have low, medium or high incomes can afford these prices without government or private insurance. Private insurers often refuse to cover these drugs.
The Liberals provided a separate $1.5 billion over three years for drugs for rare disorders, but no province or territory has signed a bilateral agreement with the federal government for these drugs and no patient has received benefit through this program. Even if they did, the $500 million per year would not go far towards the actual costs. There is at least a zero missing in the federal contribution, as the projected cost of public spending on rare disease medicines by 2025 is more than threefold what Ottawa has budgeted.
Expensive drugs for cancer and rare disorders are just as essential as basic medicines for cardiovascular diseases, diabetes, birth control, and many other common conditions. If a costly medicine will allow a person with a life-shortening disease to live longer or one with a disorder that will be severely disabling left untreated to have an improved quality of life and be a productive taxpayer, it too should be regarded as essential.
The Liberals and NDP are working to stampede the bill to introduce the pharmacare program (Bill C-64) through the legislative process. This includes inviting witnesses over the first long weekend of summer, when many Canadians are away, to appear before the parliamentary Standing Committee on Health three days later.
Too much is unknown about what will be covered (will newer drugs be covered or only older, cheaper medicines?), who will be eligible for coverage (all appropriate Canadians regardless of existing coverage or only those with no present coverage?), and what the real cost will be, including whether a new program focusing on older, cheaper drugs will deter drug developers from launching novel medicines for unmet needs in Canada.
This Bill as it stands is such a power grab that, if passed, the federal Health Minister never has to come back to Parliament for review, oversight or another tranche of legal authority, it would empower the Cabinet to make rules and regulations without parliamentary scrutiny.
A lot is at stake for Canadians, especially for patients and their doctors. Prescription medicines are of critical importance to treating many diseases. National pharmacare must not only allow low-income residents to access purported “essential medicines” but also ensure that patients who need specialized drugs, especially higher-cost innovative cell and genetic therapies that may be the only effective treatment for their disorder, are not ignored. Canadians should be careful what they wish for. They may receive less than they anticipate, and, in fact, many Canadians may be worse off despite the increase in public spending. Time to look under the hood and kick the tires.
Nigel Rawson is a senior fellow with the Macdonald-Laurier Institute.
John Adams is co-founder and CEO of Canadian PKU and Allied Disorders Inc., a senior fellow with the Macdonald-Laurier Institute and volunteer board chair of Best Medicines Coalition.


By Adam Zivo
Harm-reduction activists claim evidence supports “safer supply,” but their studies don’t back that up.
Canada, where I call home, is the only jurisdiction in the world that hands out free addictive drugs to addicts. Under the “safer-supply” policy, Canadian health authorities distribute hydromorphone—an opioid as potent as heroin—as well as, to a lesser degree, oxycodone, pharmaceutical fentanyl, and mild stimulants. These drugs are provided at no cost and, until recently, rarely had to be consumed under medical supervision.
Some American harm-reduction activists claim that Canada’s experience—and studies of it—prove that safer supply saves lives. In reality, the studies they cite are deeply flawed. They rely on weak methodologies, including biased interviews and self-reported surveys, and fail to isolate the effects of safer supply from those of other interventions. U.S. policymakers should not let such shaky evidence justify similarly misguided policies at home.
Canada piloted safer supply in 2016 with no evidence that it worked. Some clinical trials suggested that administering pharmaceutical-grade heroin under careful medical supervision could stabilize severely addicted drug users. But advocates took this evidence and claimed that it supported their safer-supply experiment, despite crucial dissimilarities—the most important being the lack of witnessed consumption.
Over the following years, radical activist-scholars produced numerous evaluations and studies declaring that safer supply “saves lives” and improves recipients’ quality of life. As Canada expanded program access nationwide in 2020, policymakers latched on to this “evidence-based” experiment, condemning critics as anti-science.
This evidence is predominantly composed of qualitative studies, which rely not on data but on interviews with safer-supply recipients and providers. The interviewees naturally say that the program is wonderful and has few downsides. Advocates then frame these responses as objective evidence of success.
Notably, the studies never reach out to those who might provide negative evaluations of safer supply—doctors, addicts uninvolved with these programs, or individuals newly in recovery. Addiction experts throughout Canada have dismissed these studies as glorified customer testimonials.
Some studies involve surveys, converting patient responses into quantitative data that can be statistically analyzed. For example, the London InterCommunity Health Centre (LIHC), one of Canada’s leading safer-supply prescribers, publishes survey-based evaluations that claim approximately half of its patients reduced their fentanyl consumption after enrollment. This quantitative method does not change the unreliability of self-reported data, however, and there’s nothing that keeps patients from giving false answers if it suits their interests.
A 2024 study conducted by Brian Conway, director of Vancouver’s Infectious Disease Centre, indirectly validated these criticisms. The study distributed surveys to 50 of his safer-supply patients and then collected urine samples immediately afterward. Conway discovered that, while only 4 percent of these patients self-reported diverting (selling or trading) all their safer-supply hydromorphone, 24 percent had no hydromorphone in their urine. That suggests a significant portion of patients lied on their surveys.

A few studies use administrative health data to show that enrollment in federally funded safer-supply programs correlates with improved health outcomes. But these studies make no effort to determine whether the free drugs themselves are responsible. The real driver could be the extensive wraparound services the programs offer, such as housing assistance and access to primary care. It’s like giving an obese man a personal trainer and a daily slice of cake—and then, when he loses weight, crediting the cake.
Last year, the British Columbia Centre for Disease Control (BCCDC) published a study in the British Medical Journal examining the health data of 5,882 drug users over an 18-month period between 2020 and 2021. The study found that individuals who received safer-supply opioids were 61 percent less likely to die over the following week than those who didn’t. This number rose to 91 percent for those receiving safer-supply opioids for four or more days in a single week.
Encouraging, right? But not so fast. When a team of seven addiction physicians reviewed the study, they discovered that the researchers misrepresented their data. Safer-supply patients are often co-prescribed traditional addiction medications, such as methadone and Suboxone, that have long been proven to reduce overdoses and deaths (these medications are often referred to as opioid agonist therapy, or OAT). The study data showed that safer-supply patients who did not also receive OAT medications were just as likely to die as those who did not get safer supply. In other words, the benefits that the BCCDC researchers touted were likely driven primarily by OAT, not safer supply.
The study data also showed no significant mortality reductions after one year of accessing safer supply. One wonders why the researchers chose to fixate on the one-week follow-up numbers.
Most recently, a study published in JAMA Health Forum found that, between 2020 and 2022, British Columbia’s safer-supply policy was associated with a 33 percent increase in opioid hospitalizations and no change to drug-related mortality. The researchers arrived at this conclusion by comparing the province’s publicly available health data with data from a control group made up of a handful of other Canadian provinces. The study raised further doubts about safer supply’s scientific basis.
Over the past two years, Canadian policymakers have openly, if reluctantly, acknowledged that safer supply is not as well-supported as they once claimed. British Columbia’s 2023 safer supply fentanyl protocols clearly state, for example, that “there is no evidence available supporting this intervention, safety data, or established best practices for when and how to provide it.” Similarly, the province’s top doctor released a report in early 2024 admitting that the experiment is “not fully evidence based.” Just last autumn, the Canadian Research Initiative in Substance Matters acknowledged in a major presentation that safer supply is supported by “essentially low-level evidence.”
This about-face has been hastened by investigative media reports confirming that safer-supply drugs were being diverted to the black market, enriching organized crime and corrupt pharmacies in the process. Public support for the policy has apparently declined, as once-taboo criticism becomes normalized among Canadian politicians and commentators. The Canadian federal government has now quietly defunded its safer-supply programs (though independent prescribers still operate), while British Columbia mandated earlier this year that all safer-supply drugs be consumed under supervision.
Harm-reduction activists nonetheless maintain that the blowback against safer supply represents a “moral panic,” and that politics is overriding evidence-based policymaking. “Safer supply saves lives! Follow the science!” they insist. International policymakers, especially in the United States, should see through these misrepresentations.
The Bureau is a reader-supported publication.
To receive new posts and support my work, consider becoming a free or paid subscriber.
Invite your friends and earn rewards

The Vigilant Fox and Overton |
This might be the biggest shake-up in American healthcare history.
President Trump just did what every other politician only talked about—he took a sledgehammer to Big Pharma. With the stroke of a pen, he signed an executive order that could slash drug prices by as much as 90%.
And then RFK Jr. stepped up and revealed why no one else—not even Bernie Sanders—ever followed through.
Standing before reporters and his healthcare team, President Trump announced the most aggressive move on drug pricing America has ever seen. The plan? To cut prescription drug costs by up to 90%—a direct strike against the industry that’s drained American families dry for years.
“Starting today, the United States will no longer subsidize the health care of foreign countries, which is what we were doing,” Trump said. “We were subsidizing others’ health care, countries where they paid a small fraction of what for the same drug that what we pay many, many times more for.”
This wasn’t just about reining in corporate greed. Trump laid it out clearly: this was a global scam, and America was the one footing the bill.
“And [we] will no longer tolerate profiteering and price gouging from Big Pharma,” he added. “But again, it was really the countries that forced Big Pharma to do things that frankly, I’m not sure they really felt comfortable doing, but they’ve gotten away with it, these countries, European Union has been brutal, brutal.”
Trump promised that would change. “So for the first time in many years, we’ll slash the cost of prescription drugs and we will bring fairness to America.”
How much cheaper? “If you think of a drug that is sometimes ten times more expensive, it’s much more than the 59%… but between 59 and 80, and I guess even 90%.”
For struggling families, this wasn’t just reform. It was real relief.
Then came the reveal that changed everything. HHS Secretary Robert F. Kennedy Jr. stood beside the president and exposed one of Washington’s best-kept secrets. It wasn’t just corruption—it was betrayal.
“This is an extraordinary day,” Kennedy began. “This is an issue that, you know, I grew up in the Democratic Party, and every major Democratic leader for 20 years has been making this promise to the American people.”
He pointed straight to Bernie Sanders, who made drug pricing the core of his presidential campaigns. “This was the fulcrum of Bernie Sanders runs for presidency, that he was going to eliminate this discrepancy between Europe and the United States.”
But none of them actually meant to fix it.
“As it turns out, none of them were doing it. And it’s one of these promises that politicians make to their constituents, knowing that they’ll never have to do it.”
Why not? Because the system was never meant to be fixed.
“There’s at least one pharmaceutical lobbyist for every congressman, every Senator on Capitol Hill, and every member of the Supreme Court,” Kennedy said.
“There has never been a president more willing to stand up to the oligarchs than President Donald Trump,” he added. “And I’m very, very proud of you, Mr. President, for your courage, for I’ll say it because I don’t want to be crude, your intestinal fortitude, your stiff spine and your willingness to stand up for the American people.”
With one line, RFK Jr. shattered the bipartisan charade—and gave Trump credit no Democrat had the guts to say out loud.
If you’re not following me yet, you’re missing the real story behind the headlines.
I post critical updates daily. Subscribe now and stay ahead of the curve.
Then Dr. Oz came with a line that hit hard.
“This is the most powerful executive order on pharmacy pricing and healthcare ever in the history of our nation.”
He explained how Americans were stuck paying five to ten times more than Europeans for the exact same drugs—and why that ends now.
“It’s only happening because we have a president with the fortitude, the guts to stand up to the withering criticism and lobbying that’s going to occur as soon as folks hear about the executive order,” said the head of CMS.
Dr. Oz made it personal. “On behalf of the child in Philadelphia with a $1,000-a-month drug, or the older woman in L.A. who can’t afford her blood thinner—I’m going to thank President Trump. God bless you for having the guts to take on this industry.”
He said Trump’s plan will force other countries to start paying their fair share, just like with NATO.
“When President Trump said you’ve got to pay a little more, they came up. The same thing we believe will happen here.”
Negotiations with drug companies start in 30 days. For the first time ever, prices will be tied to global benchmarks.
“We’re going to be able to get the pharmaceutical industry whole—and finally pay the appropriate amount.”
Then NIH Director Jay Bhattacharya took the mic and called it what it was: long overdue.
“What President Trump has done is a historic measure that should have been done a long time ago.”
He explained the economics behind the scam. “One thing that’s really, really simple in economics is that when you have a persistent price difference for the same product between two countries, there’s something deeply wrong.”
Bhattacharya said Americans were being used to fund global research and development, and that ends now.
“Right now, what’s happening is the American people are subsidizing, in a large fraction, the research and development efforts for drug companies around the world, by the higher prices that we pay.”
“With this new order, Europe will share the burden of that.”
This wasn’t new information. The facts have been known for decades. But no one acted—until now.
“We’re standing up for the American consumer who’s been paying far too high prices for far too long.”
“And nothing has been done about it until this moment.”
He turned to the president and said, “I’m really, really proud, President Trump, that you have done this, and I’m really proud to be included in this and looking forward to the work ahead.”
And just before signing, Trump made it clear: Democrats were now in a tough spot.
“We’re now, on top of the tax cuts and regulation cuts, all the things, now you’re going to say that the price of your medicine is going down by 60, 70, 80%. You’re going to vote against it?”
“I think a lot of Democrats will be forced to do something that their leaders are going to beg them not to do, and that’s vote for the bill.”
“I don’t see how they can vote against it.”
That’s when ABC jumped in with a question about a jet from Qatar, implying it was a personal gift to Trump.
Without skipping a beat, Trump fired back. “You’re ABC fake news, right?”
“Let me tell you, you should be embarrassed asking that question. They’re giving us a free jet. I could say no, no, no. Don’t give us. I want to pay you a billion or $400 million or whatever it is. Or I can say thank you very much.”
When she pressed again, Trump hit even harder.
“It’s not a gift to me, it’s a gift to the Department of Defense. You should know better. Because you’ve been embarrassed enough, and so has your network.”
“Your network is a disaster. ABC is a disaster,” Trump added.
Finally, Trump lifted the bill and called Kennedy up beside him. “Here is the bill, Bobby, come on over here.”
Thanks for reading! This post took time and care to put together, and we did our best to give this story the coverage it deserved.
If you like my work and want to support me and my team and help keep this page going strong, the most powerful thing you can do is sign up for the email list and become a paid subscriber.
Your monthly subscription goes further than you think. Thank you so much for your support.



Premier Smith seeks Alberta Accord: Announces new relationship with Ottawa
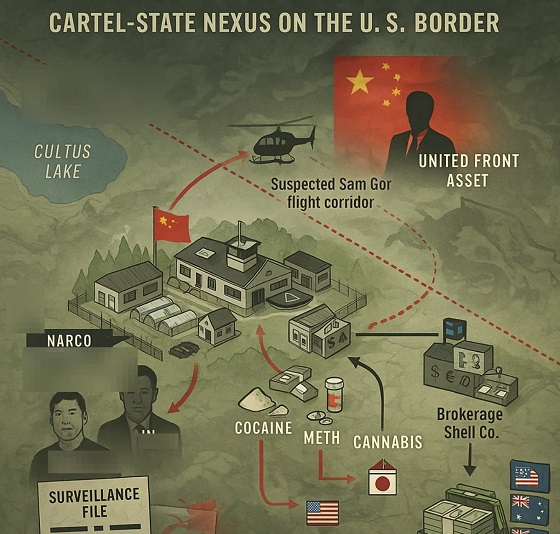
Inside B.C.’s Cultus Lake Narco Corridor — How Chinese State-Linked Syndicates are Building a Narco Empire in Canada

Ice Surprises – Arctic and Antarctic Ice Sheets Are Stabilizing and Growing

It’s time to get excited about the great Canadian LNG opportunity
-
 Alberta2 days ago
Alberta2 days agoAlberta’s oil bankrolls Canada’s public services
-
 Great Reset22 hours ago
Great Reset22 hours agoThe WHO Pandemic Treaty could strip Canada of its ability to make its own health decisions
-
 Business2 days ago
Business2 days agoThe ESG Shell Game Behind The U.S. Plastics Pact
-
 International2 days ago
International2 days agoBongino announces FBI will release files on COVID cover up, Mar-a-Lago Raid and more
-
 Fraser Institute21 hours ago
Fraser Institute21 hours agoCarney government’s housing plan poses major risks to taxpayers
-
 espionage21 hours ago
espionage21 hours agoPro-Beijing Diaspora Group That Lobbied to Oust O’Toole Now Calls for Poilievre’s Resignation Amid PRC Interference Probes
-
 espionage15 hours ago
espionage15 hours agoOttawa Raises Alarm With Beijing Over Hong Kong Detention of CPC Candidate Joe Tay’s Family
-
Health15 hours ago
RFK Jr. Says Trump Just Did What No Democrat Ever Had the Guts to Do